&geometry(187x114) "ESANZ")
APSC 2026 Consensus on TEER for Tricuspid and Mitral Regurgitation
Asia Pacific Society of Cardiology publishes their new Consensus on TEER for Tricuspid and Mitral Regurgitation
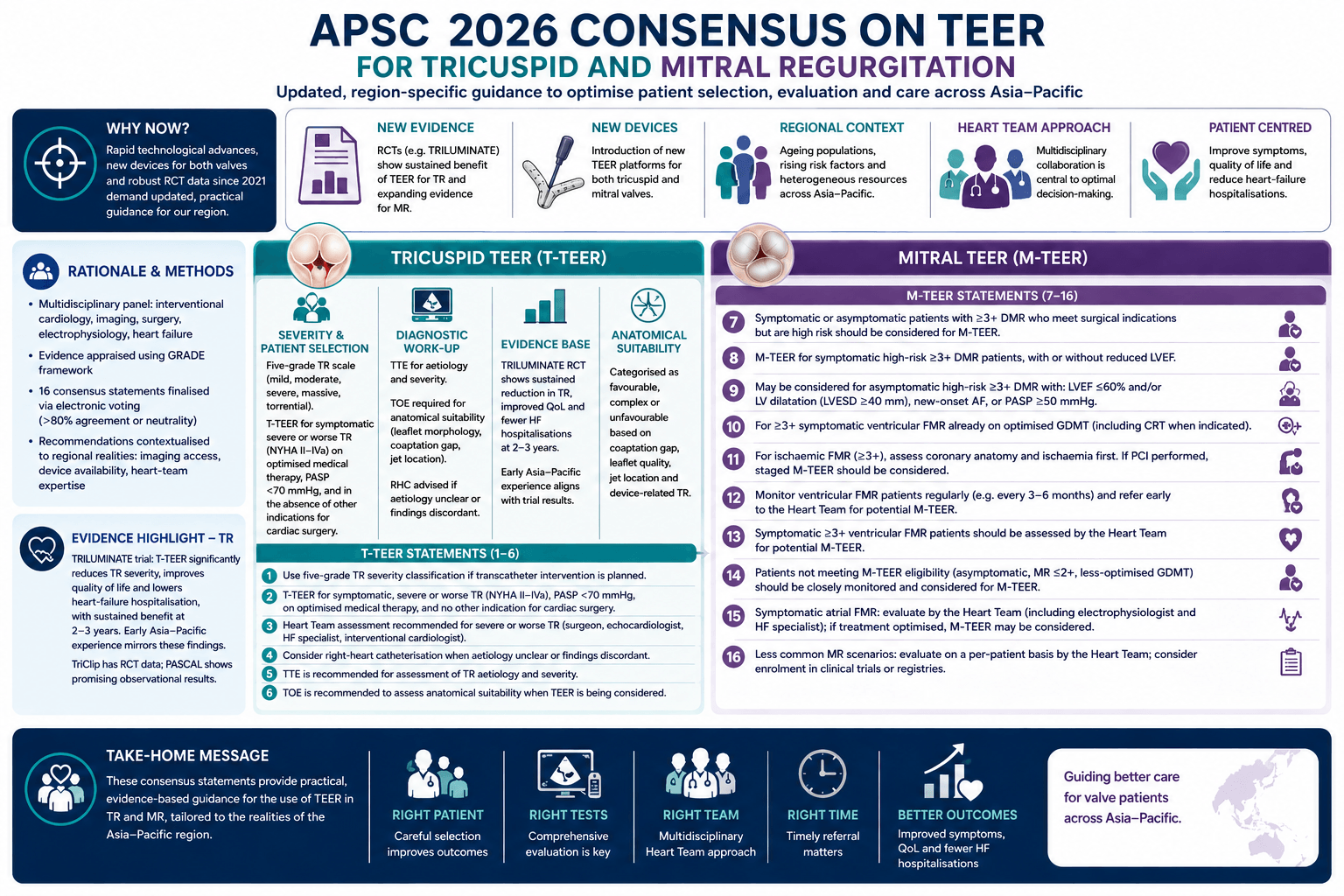
The 2026 Asian Pacific Society of Cardiology (APSC) consensus statement provides updated, region-specific guidance on the use of transcatheter edge-to-edge repair (TEER) for tricuspid regurgitation (TR) and mitral regurgitation (MR). This update follows rapid technological expansion since the 2021 MitraClip-focused consensus, including the introduction of new TEER devices for both valves and the emergence of robust randomised trial data. The document aims to support general cardiologists and internal medicine specialists across the Asia-Pacific region, where ageing populations, rising cardiovascular risk factors, and heterogeneous healthcare resources create unique challenges in valvular disease management: assets.radcliffecardiology.com
Rationale and Methods
The panel comprised experts in interventional cardiology, imaging, surgery, electrophysiology, and heart failure. Evidence was appraised using the GRADE framework, and 16 consensus statements were finalised after electronic voting requiring >80% agreement or neutrality. The recommendations emphasise contextualisation to regional realities, including variable access to advanced imaging, device availability, and heart-team expertise.
Tricuspid TEER
1. Severity Classification and Patient Selection
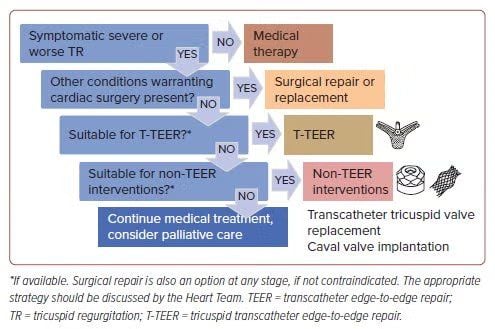
The panel endorses the five-grade TR severity scale (mild, moderate, severe, massive, torrential), which offers better risk stratification than the traditional four-tier system. T-TEER is recommended for symptomatic severe or worse TR (NYHA II-IVa) with pulmonary artery systolic pressure <70 mmHg on optimised medical therapy, and in the absence of other indications for cardiac surgery.
2. Diagnostic Work-up
- TTE is recommended for assessing TR aetiology and severity.
- TOE is required to determine anatomical suitability, particularly leaflet morphology, coaptation gap, and jet location.
- Right-heart catheterisation is advised when aetiology is unclear or non-invasive findings are discordant.
3. Evidence Base
The TRILUMINATE pivotal trial demonstrated that T-TEER significantly reduces TR severity, improves quality of life, and lowers heart-failure hospitalisation compared with medical therapy alone, with sustained benefit at 2-3 years. Early Asia-Pacific experience mirrors these findings. The TriClip system remains the only platform with randomised data, though PASCAL shows promising observational results.
4. Anatomical Suitability
Anatomy is categorised as favourable, complex, or unfavourable based on coaptation gap, leaflet quality, jet location, and presence of device-related TR. This framework supports reproducible patient selection across diverse centres.
Tricuspid TEER Statements
The guideline committee produced the followng statements regarding transcatheter tricuspid repair.
Statement 1. If transcatheter intervention is planned, the five-grade classification of TR severity is recommended.
Statement 2. In the absence of other conditions requiring cardiac surgery, T-TEER should be considered for symptomatic, severe or worse TR if the following criteria are met: New York Heart Association class II-IVa HF symptoms, pulmonary artery systolic pressure <70 mmHg and on optimised medical therapy.
Statement 3. Assessment by a multidisciplinary Heart Team is recommended in patients with clinically significant severe or worse TR; the team should include, at a minimum, a heart surgeon, echocardiologist, HF specialist and interventional cardiologist.
Statement 4. Right-heart catheterisation should be considered in patients with severe or worse TR when the aetiology is unclear or findings are discordant, to clarify contributions of left-sided disease or pulmonary hypertension and to define haemodynamic severity.
Statement 5. Transthoracic echocardiography is recommended for assessment of TR aetiology and severity.
Statement 6. If TEER is being considered, transoesophageal echocardiography (TOE) is recommended to assess anatomical suitability.
Mitral TEER Statements
The guidline committee decided upon the following position statements for M-TEER.
Statement 7. Both symptomatic and asymptomatic patients with >=3+ DMR, who meet the indications for surgery but are considered high risk by the Heart Team, should be considered for M-TEER.
Statement 8. M-TEER should be considered for symptomatic highrisk >=3+ DMR patients with or without reduced left ventricular (LV) ejection fraction (LVEF).
Statement 9. M-TEER may be considered for asymptomatic patients with high-risk >=3+ DMR, with: reduced LVEF (<=60%) and/or LV dilatation (LV end-systolic diameter >=40 mm), new-onset AF or pulmonary hypertension (systolic pulmonary arterial pressure >=50 mmHg).
Statement 10. M-TEER should be considered for (>=3+) symptomatic ventricular FMR patients who are already receiving optimised GDMT, including cardiac resynchronisation therapy when indicated.
Statement 11. For ischaemic FMR (>=3+), coronary anatomy and ischaemia evaluation should be performed before M-TEER consideration. If percutaneous coronary intervention is performed, staged M-TEER therapy should be considered for severe symptomatic FMR..
Statement 12. Ventricular FMR patients should be monitored regularly (e.g. every 3-6 months) and referred early to the Heart Team (including a TEER specialist, HF specialist, echocardiologist and surgeon) for potential M-TEER.
Statement 13. Symptomatic patients with >=3+ ventricular FMR should be assessed by the Heart Team for potential M-0TEER.
Statement 14. Ventricular FMR patients who do not meet the eligibility criteria for M-TEER (e.g. asymptomatic patients, those with MR severity of <=2+, and those with less-optimised GDMT) should be closely monitored. These patients should be considered for M-TEER.
Statement 15. Patients with symptomatic atrial FMR should be evaluated by the Heart Team (including an electrophysiologist and HF specialist) and, if treatment has already been optimised, M-TEER may be considered.
Statement 16. Patients with less common scenarios of MR should be evaluated by the Heart Team on a per-patient basis to determine whether M-TEER use would be feasible and beneficial for them. Enrolment into clinical trials or registries should be considered.
)