&geometry(187x114) "ESANZ")
Beyond RVSP: The New Era of Echo Assessment in Pulmonary Hypertension
Bonita Anderson present this first of her two-part series of Echo in pulmonary hypertension.
Beyond RVSP: The New Era of Echo Assessment in Pulmonary Hypertension
Pulmonary hypertension (PH) is a progressive and potentially life-threatening condition that places significant strain on the right side of the heart. Because symptoms such as breathlessness and fatigue are often non-specific, early recognition can be challenging. Delayed diagnosis may lead to worsening right ventricular (RV) dysfunction, heart failure, and increased mortality.
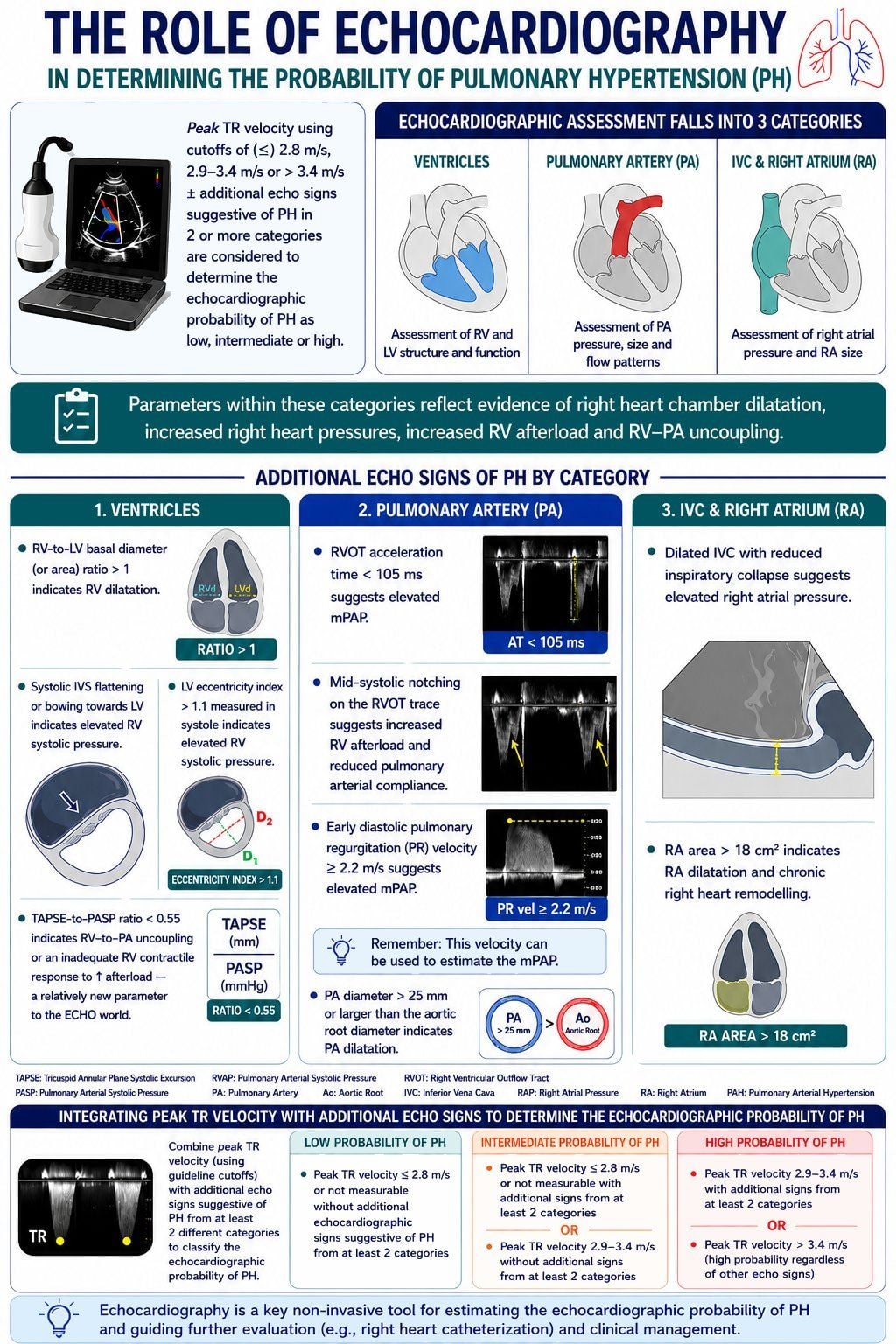
Although the gold standard for diagnosing PH remains right heart catheterization (RHC), not every patient with unexplained dyspnoea or suspected PH should immediately undergo invasive testing. This is where echocardiography plays a crucial role.
Today, echocardiography is no longer just about estimating pulmonary pressures — it now involves a comprehensive, multiparametric assessment of the right heart and pulmonary circulation.
Why Echocardiography Is Important
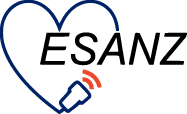
Echocardiography is recommended as the first-line, non-invasive test for evaluating suspected PH as it provides valuable information about:
- Estimation of pulmonary and right heart pressures
- Right ventricular size and function
- RV adaptation to increased afterload
Traditionally, we have focused heavily on the estimated right ventricular systolic pressure (RVSP) or pulmonary artery systolic pressure (PASP). However, recent guidelines emphasize that the peak tricuspid regurgitation (TR) velocity — rather than the calculated RVSP/PASP — is the key variable used to assess the echocardiographic probability of PH. This is because echo-derived PASP may differ from invasive measurements obtained during RHC. In addition, TR velocity alone cannot reliably confirm or exclude PH since it is influenced by technical and haemodynamic factors.
Therefore, echocardiographic assessment of PH now requires a broader multiparametric approach.
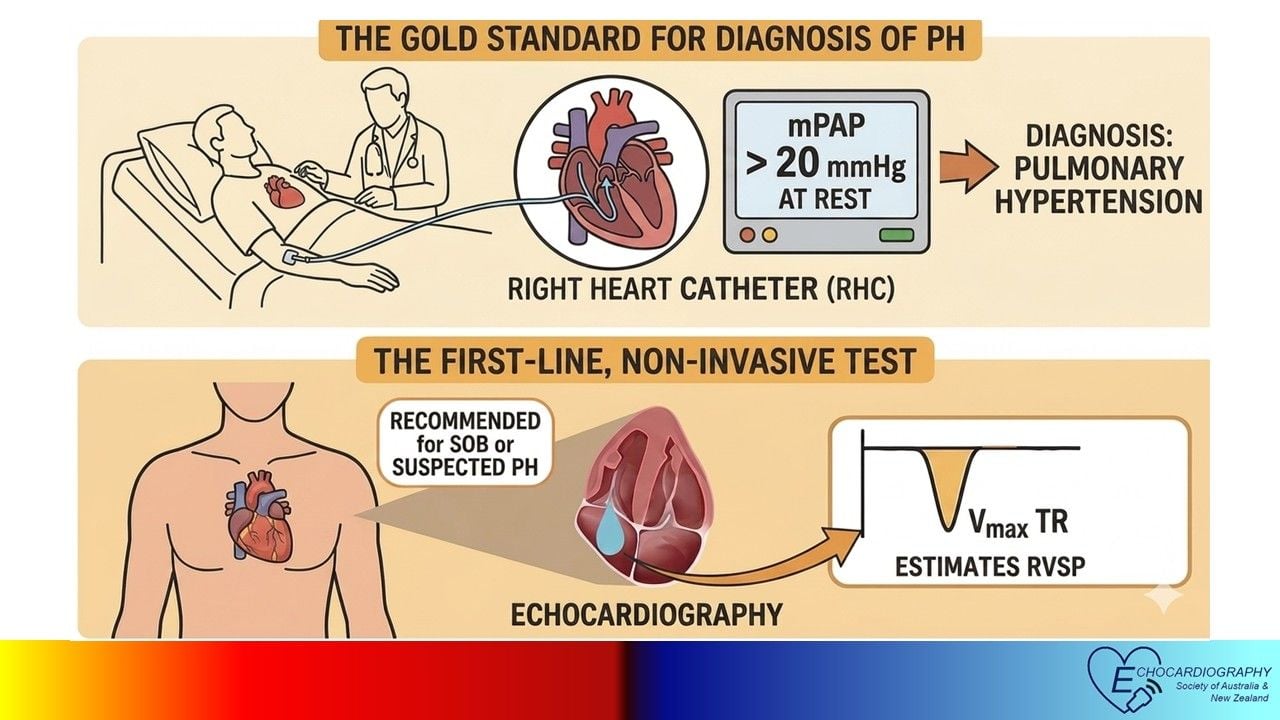
Echocardiographic Probability of PH
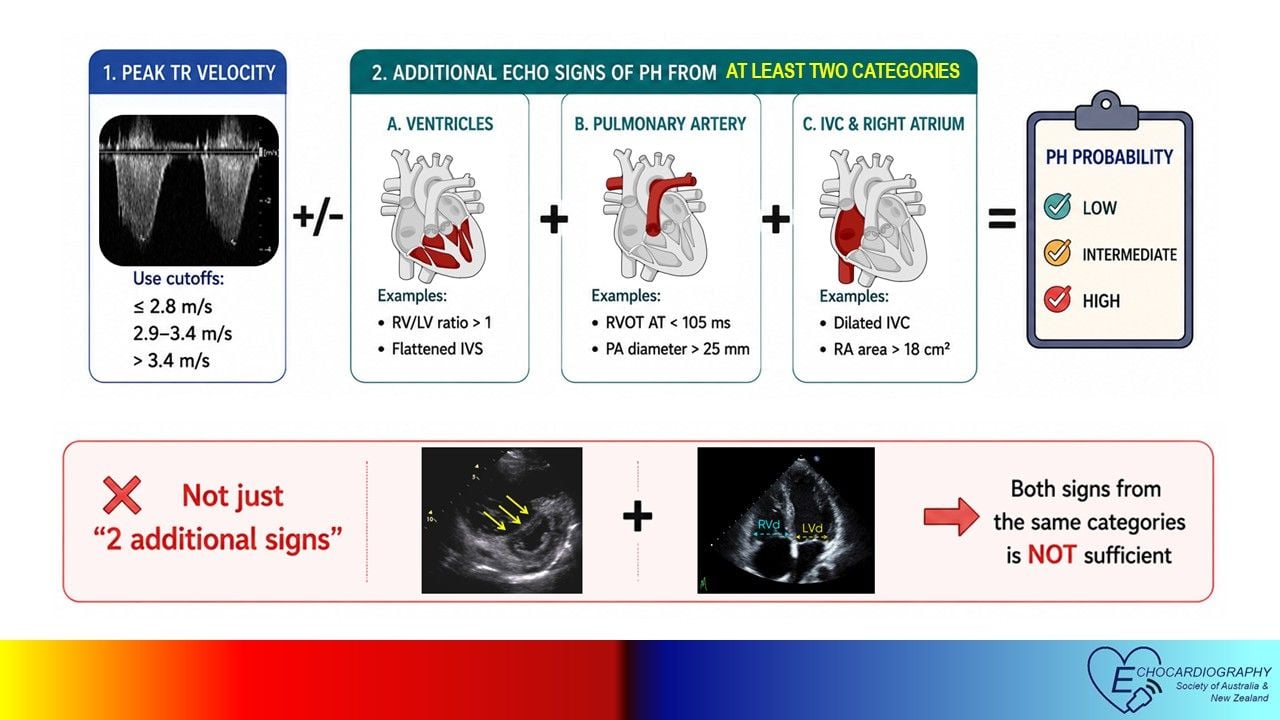
Current guidelines recommend combining the peak TR velocity with additional echocardiographic signs suggestive of PH. Importantly, these additional findings should be present across at least two different echocardiographic categories — rather than simply identifying two abnormal findings from the same category.
Low Probability
- Peak TR velocity <=2.8 m/s or not measurable without additional echo signs suggestive of PH from at least two categories
Intermediate Probability
- Peak TR velocity <=2.8 m/s or not measurable with additional echo signs from at least two categories
OR
- Peak TR velocity 2.9-3.4 m/s without additional echo signs from at least two categories
High Probability
- Peak TR velocity 2.9-3.4 m/s with additional echo signs from at least two categories
OR
- Peak TR velocity >=3.4 m/s (indicates a high probability of PH regardless of other echo signs).
Additional Echo Signs of PH
Additional signs of PH are grouped into three categories.
1. Ventricular Signs
- RV-to-LV basal diameter ratio > 1 suggests RV dilatation
- Systolic septal flattening or LV eccentricity index >=1.1 indicates elevated RV systolic pressure
- TAPSE-to-PASP ratio <=0.55 suggests RV-PA uncoupling and impaired RV adaptation to increased afterload
2. Pulmonary Artery Signs
- RVOT acceleration time <=105 ms suggests elevated mPAP
- Mid-systolic notching indicates increased RV afterload and reduced pulmonary arterial elasticity
- Early diastolic PR velocity >=2.2 m/s reflects elevated mPAP
- PA diameter >=25 mm or larger than the aortic root suggests PA dilatation due to chronic pressure overload
3. IVC and Right Atrial Signs
- Dilated IVC with reduced inspiratory collapse suggests elevated right atrial pressure (RAP)
- Right atrial area >=18 cm² indicates RA dilatation and chronic right heart remodelling
Importantly, additional echo signs must span at least two different categories to raise the probability of PH. The presence of two additional signs alone is insufficient if both are derived from the same category.
Key Takeaways
- Echocardiography is the first-line imaging test for suspected PH.
- RHC remains the gold standard for definitive diagnosis.
- Today’s PH assessment is not based on RVSP/PASP alone.
- Peak TR velocity should be integrated with additional echocardiographic signs identified across at least two different categories.
Ultimately, echocardiography in PH assessment is not simply estimating RVSP/PASP — it is assessing the interaction between the right heart and pulmonary circulation, helping identify patients who require further investigation.
References and Further Readings
Humbert M, Kovacs G, Hoeper MM, et al; ESC/ERS Scientific Document Group.
2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary
hypertension. Eur Respir J. 2023 Jan 6;61(1):2200879.
Mukherjee M, Rudski LG, Addetia K, et al. Guidelines for the Echocardiographic
Assessment of the Right Heart in Adults and Special Considerations in Pulmonary
Hypertension: Recommendations from the American Society of Echocardiography. J
Am Soc Echocardiogr. 2025 Mar;38(3):141-186.
)