&geometry(187x114) "ESANZ")
Diastology Guidelines - the new and the old...
The 2025 Diastolic Function Algorithm in the Real World
The 2016 ASE diastolic guidelines used a single-step majority rule, requiring at least two of three criteria (E/e', TRVmax, LAVi) to define elevated left atrial pressure, with discordant findings falling into an "indeterminate" bucket. The 2025 ASE Diastology Guidelines update takes a fundamentally different approach: a two-step algorithm where primary Doppler indices (e', E/e', TRVmax) classify filling pressure when concordant, and secondary markers (PV S/D, LARS, LAVi) adjudicate when they're not. On paper, indeterminate no longer exists.
A recent paper by Spetko et al. assessed the impact on these new 2025 guidelines in the diagnostic reclassification of patients.
Evaluating almost 13,000 echocardiograms, the 2025 algorithm reclassified one in four patients compared to 2016 criteria. Indeterminate rates dropped from 15.3% to 10.4%, and mortality discrimination improved modestly but significantly (AUC 0.65 vs 0.63, p=0.03). The finding that patients reclassified as having diastolic dysfunction by both algorithms carried the highest mortality is an important signal, with concordance across guidelines identifying a genuinely high-risk group.
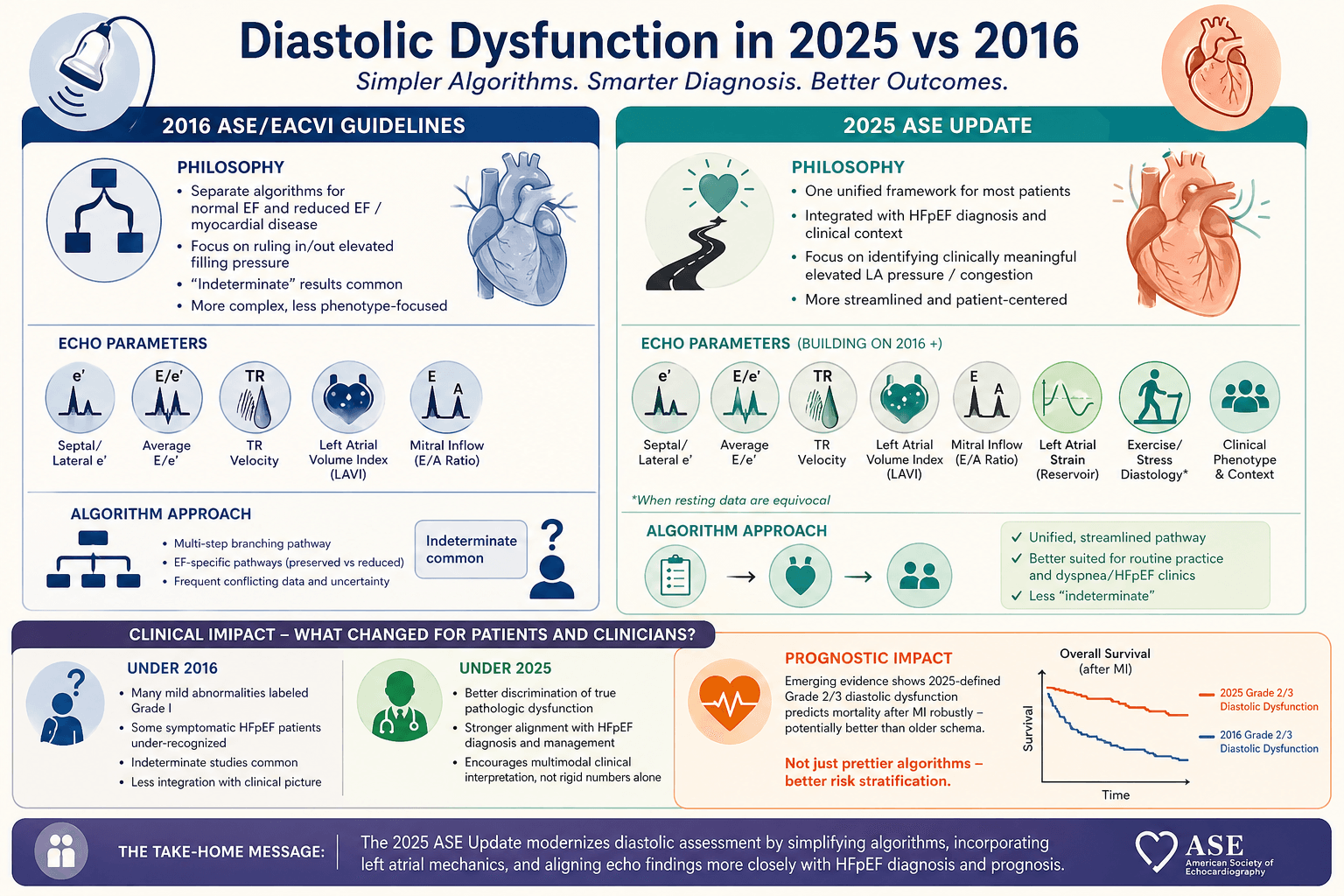
One of the key issues that remains is the rate of missing data. Indeed, the authors highlighted the missingness of important parameters including left atrial reservoir strains (LARS), pulmonary vein systolic/diastolic velocity ratio and isovolumetric relaxation time (IVRT). These adjudicating parameters may add both diagnostic and prognostic value; without them, indeterminate rates remain higher than optimal.
Overall, this study suggests a clear improvement in the utility of such guidelines in the work-up of diastolic dysfunction, however their real-world performance may only match their potential once labs collect the data to support them.
Spetko et al., J Am Soc Echocardiogr 2026 (Article in Press).
)