&geometry(187x114) "ESANZ")
ESANZ History Series: The Carpentier Classification Systems
Carpentier classification for valvular regurgitation
In 1983, Dr Alain Carpentier introduced a landmark “functional approach” to mitral regurgitation (MR) in his seminal Cardiac Valve Surgery address on Cardiac valve surgery--the "French correction" (J Thorac Cardiovasc Surg 86:323-337, 1983). In that address, he introduced a principle that continues to shape modern valve repair surgery: “Surgeons are not basically concerned with lesions. We care more about function. Therefore, one may define the aim of a valve reconstruction as restoring normal valve function rather than normal valve anatomy.”
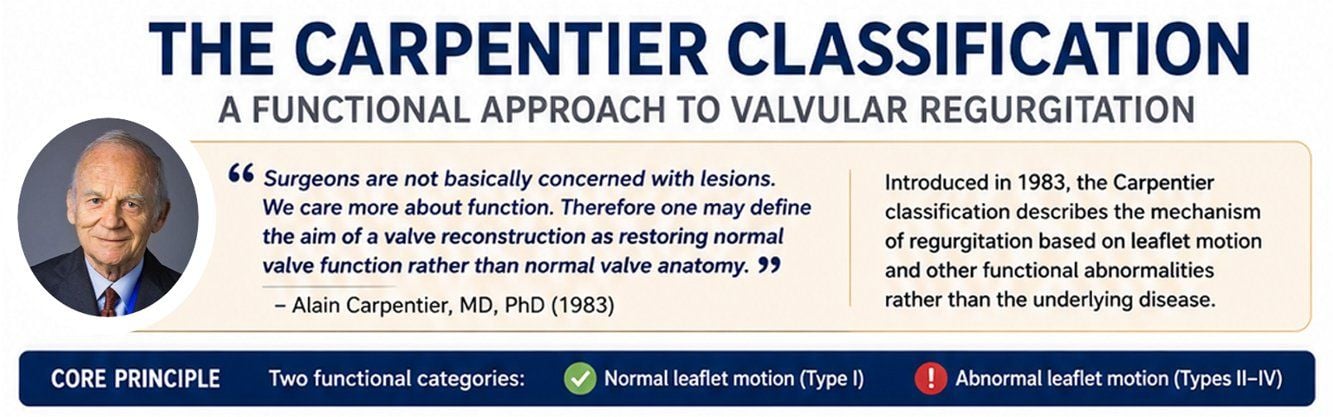
This philosophy shifted the focus of valvular assessment away from purely anatomical abnormalities and toward the functional mechanism responsible for regurgitation. The original Carpentier classification, developed as a framework to guide mitral valve repair or replacement, categorized MR according to leaflet motion. It distinguished between normal leaflet motion (Type I) and abnormal leaflet motion, either excessive motion due to prolapse (Type II) or restricted motion (Type III).
Over time, the classification has evolved, but its central concept remains unchanged: MR should be understood according to the functional behaviour of the valve leaflets. This classification has since been modified and now includes the following categories:
- Type I MR - Normal leaflet motion, typically associated with annular dilatation or leaflet perforation.
- Type II MR - Excessive leaflet motion, most commonly due to mitral valve prolapse (MVP) or chordal rupture.
- Type IIIa MR - Restricted leaflet opening and closure, classically seen in rheumatic mitral valve disease.
- Type IIIb MR - Restricted leaflet closure, usually secondary to left ventricular remodelling in ischaemic heart disease.
- Type IV MR - Systolic anterior motion (SAM) of the mitral valve, often associated with hypertrophic obstructive cardiomyopathy.
- Type V MR - Mixed pathology, involving features of more than one Carpentier type.
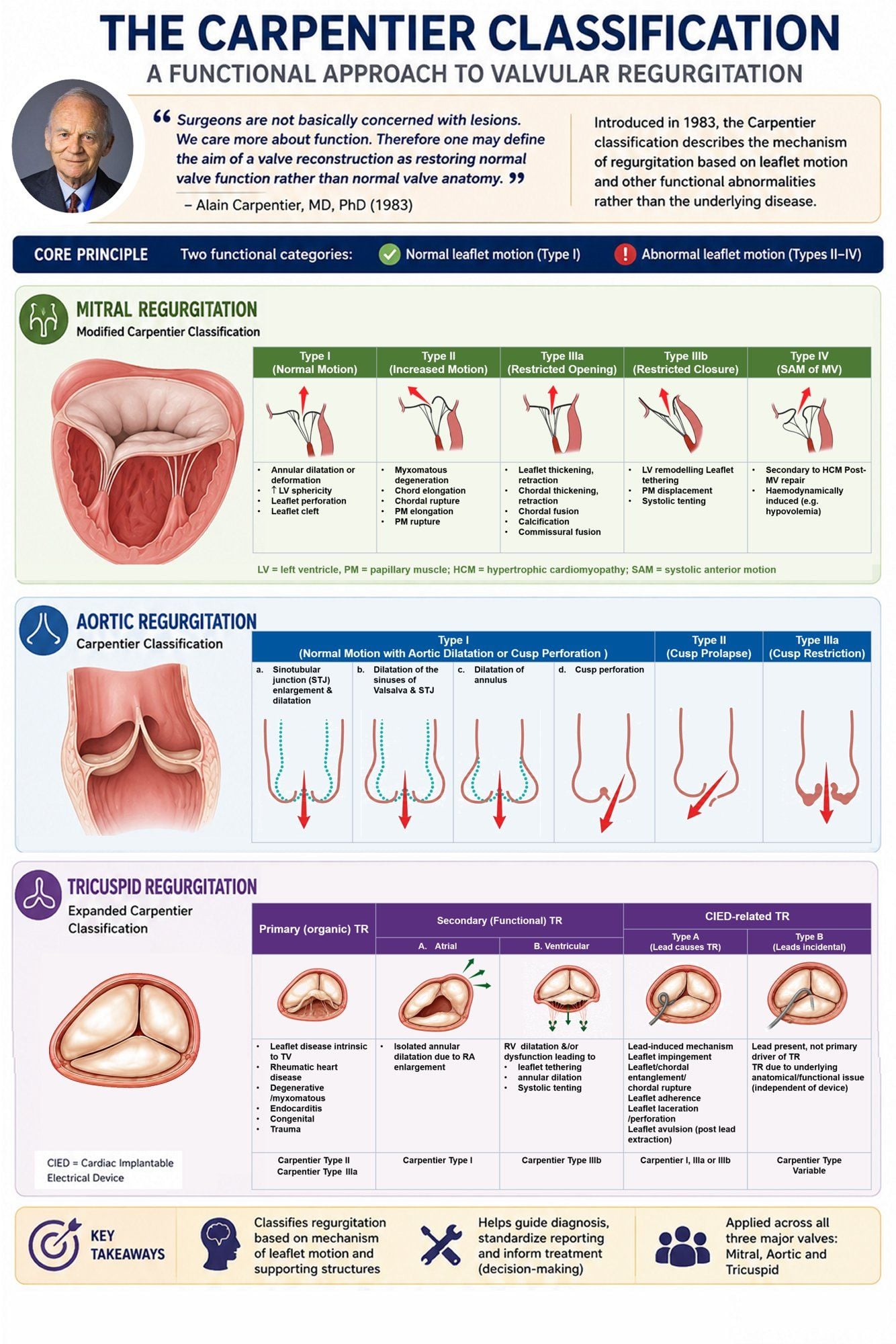
The Carpentier functional approach has since been extended beyond the mitral valve and adapted to other forms of valvular regurgitation, including aortic regurgitation (AR) and tricuspid regurgitation (TR).
For aortic regurgitation (AR), a functional classification has also been developed to guide surgical decision-making and valve repair strategies. Similar to the Carpentier approach for mitral regurgitation, AR is categorized according to cusp motion and the underlying mechanism of regurgitation.
- Type I AR - Normal cusp motion, with regurgitation resulting from pathology of the aortic root or annulus. This group can be further subdivided according to the site of dilatation or structural abnormality:
- Type Ia - Enlargement of the sinotubular junction with associated ascending aortic dilatation.
- Type Ib - Dilatation of the sinuses of Valsalva and sinotubular junction.
- Type Ic - Dilatation of the ventriculoarterial junction (aortic annulus).
- Type Id - Cusp perforation or fenestration without a primary functional annular abnormality.
- Type II AR - Excessive cusp motion resulting from cusp prolapse, typically caused by redundant leaflet tissue or commissural disruption.
- Type III AR - Restricted cusp motion due to cusp retraction or impaired leaflet mobility. This is commonly seen in congenital, rheumatic, or degenerative valve disease, as well as in conditions associated with leaflet thickening, fibrosis, or calcification.
In tricuspid regurgitation (TR), defining the underlying morphological and functional mechanism is increasingly important, particularly in the era of transcatheter tricuspid interventions. The Carpentier framework has therefore also been applied to TR.
Secondary (functional) TR is substantially more common than primary (organic) TR and is now further divided into:
- Ventricular secondary TR - Associated with right ventricular enlargement and leaflet tethering, corresponding to Carpentier Type IIIb (restricted closure).
- Atrial secondary TR - Associated with right atrial enlargement and isolated annular dilatation, corresponding to Carpentier Type I (normal leaflet motion with annular dilatation).
The growing prevalence of cardiac implantable electronic devices (CIEDs) has led to further refinement of the classification system. When a CIED lead directly causes TR through leaflet impingement, entanglement, perforation, or altered right ventricular mechanics resulting in tethering, this is termed Type A CIED-related TR. Depending on the mechanism, it may manifest as:
- Type I - Normal leaflet motion,
- Type IIIa - Restricted systolic leaflet motion, or
- Type IIIb - Restricted systolic and diastolic leaflet motion.
By contrast, Type B CIED-incidental TR refers to cases in which a device lead is present but is not the primary driver of regurgitation. In these situations, TR is usually related to underlying structural or functional cardiac disease independent of the device itself.
Primary (organic) TR results from intrinsic leaflet pathology, including prolapse, degenerative disease, endocarditis, trauma, or rheumatic disease. Functionally, prolapse corresponds to Carpentier Type II, whereas rheumatic involvement is generally categorized as Type IIIa.
More than four decades after its introduction, the Carpentier classification remains one of the most influential conceptual frameworks in valvular heart disease. By emphasizing valve function over anatomy alone, it continues to guide imaging interpretation, surgical planning, transcatheter intervention, and multidisciplinary decision-making across the mitral, aortic, and tricuspid valves.
References/Further reading:
Carpentier A. Cardiac valve surgery--the "French correction". J Thorac Cardiovasc Surg. 1983 Sep;86(3):323-37.
Hahn RT, Lawlor MK, Davidson CJ, et al. Tricuspid Valve Academic Research Consortium Definitions for Tricuspid Regurgitation and Trial Endpoints. Eur Heart J. 2023 Nov 14;44(43):4508-4532.
Koo HJ, Kang JW, Kim JA, et al. Functional classification of aortic regurgitation using cardiac computed tomography: comparison with surgical inspection. Int J Cardiovasc Imaging. 2018 Aug;34(8):1295-1303.
Lebehn M, Vahl T, Kampaktsis P, Hahn RT. Contemporary Evaluation and Clinical Treatment Options for Aortic Regurgitation. J Cardiovasc Dev Dis. 2023 Aug 25;10(9):364.
Fallahtafti P, Bahramrafiee R, Sattarzadeh Badkoubeh R, et al. Revisiting Echocardiographic Ranges of Left Ventricular End-Diastolic Volume Index: An Analysis of the Discrepancies Between the 2006 and the 2015 Recommendation for Chamber Quantification Guidelines. Clin Cardiol. 2024 Sep;47(9):e70003.
Praz F, Muraru D, Kreidel F, et al. Transcatheter treatment for tricuspid valve disease. EuroIntervention. 2021 Nov 19;17(10):791-808.
Sidebotham DA, Allen SJ, Gerber IL, Fayers T. Intraoperative transesophageal echocardiography for surgical repair of mitral regurgitation. J Am Soc Echocardiogr. 2014 Apr;27(4):345-66.
Zoghbi WA, Adams D, Bonow RO, et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2017 Apr;30(4):303-371.
)