&geometry(187x114) "ESANZ")
ESANZ History Series: The Sievers Classification 2007
The Sievers Classification That Still Shapes How We Think About the Bicuspid Aortic Valve
Prior to 2007, the description of bicuspid aortic valve (BAV) morphology varied considerably across surgical and research literature. Clinicians used combinations of cusp size, sinus number, and commissural anatomy interchangeably, without a unifying framework. This was a problem that made cross-study comparisons difficult and surgical planning inconsistent for a condition affecting nearly 2% of the general population.
In 2007, Sievers and Schmidtke addressed this directly. Published in the Journal of Thoracic and Cardiovascular Surgery, their classification system was derived from 304 surgical specimens collected prospectively over five years at a single centre. The system is built around three characteristics: the number of raphes, their spatial position, and the functional status of the valve. The primary category "type" was designed to stand independently. Type 0 describes the purely bicuspid valve with no raphe, present in only 7% of cases. Type 1, with a single raphe, accounts for 88% of surgical specimens, with the left-right coronary cusp position (Type 1, L/R) representing the dominant phenotype. Type 2, carrying two raphes, is uncommon (5%) but was notably associated with a significantly higher rate of ascending aortic aneurysm, a finding that has since informed surveillance and operative decision-making.
The downstream clinical utility has been substantial. The classification provides a reproducible basis for planning valve repair versus replacement, guides proximal suture line strategy during the Ross procedure, and in the TAVR era, has become relevant to understanding how raphe calcification and annular geometry influence device selection and procedural outcomes in bicuspid anatomy.
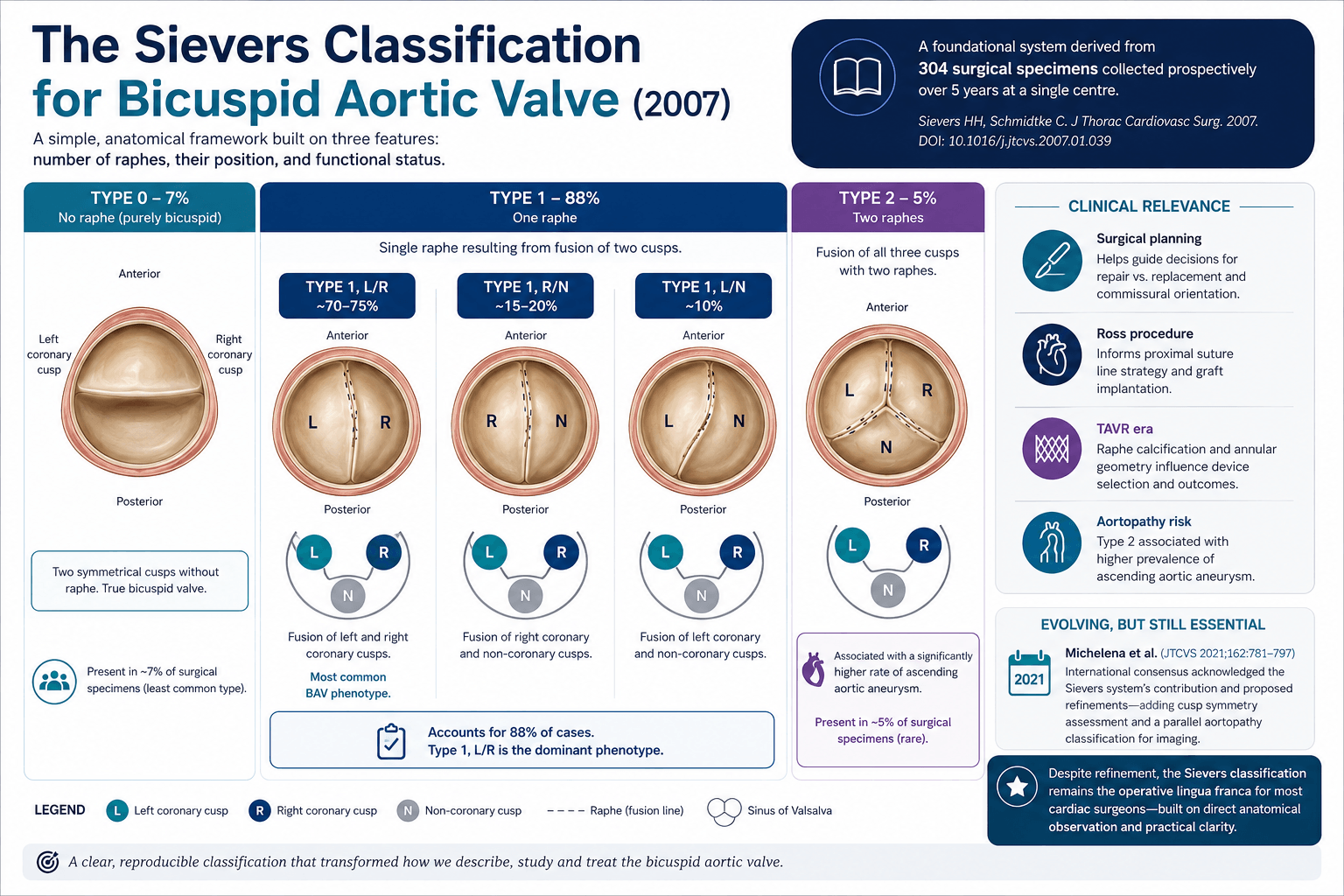
The field's acknowledgment of Sievers' contribution is perhaps best illustrated by what came next. In 2021, Michelena et al. published an international consensus statement (J Thorac Cardiovasc Surg 2021;162:781-797), co-endorsed by the STS, AATS, and EACTS and simultaneously published across four major cardiothoracic journals. It built on the Sievers classification by proposing an updated framework with a parallel aortopathy classification, as well as addressing limitations around cusp symmetry assessment, now recognised as important for repair planning.
At the guideline level, BAV morphology informed by Sievers classification is now explicitly referenced in clinical decision-making around the 2020 ACC/AHA Valvular Heart Disease Guidelines, particularly in determining suitability for TAVR versus surgical intervention, where Type 0 morphology with severe LVOT calcification is recognised as a factor favouring surgical referral. Overall, the Sievers classification remains the operative standard for most cardiac surgeons, reflecting the practical clarity of a system built from direct anatomical observation.
)